
Ectopic Pregnancy
Revised 2014
INTRODUCTION
The diagnosis of an ectopic pregnancy is usually unexpected and is often emotionally traumatic. Many women may have only recently discovered they were pregnant when they received the diagnosis. Some women diagnosed with an ectopic pregnancy do not even know they are pregnant and suddenly must think about the possibility of major surgery or medical treatment. This booklet is designed to provide information on the diagnosis and treatment of ectopic pregnancy.
Definition
Ectopic pregnancies account for 1% to 2% of all conceptions. An ectopic pregnancy is an early embryo (fertilized egg) that has implanted outside of the uterus (womb), the normal site for implantation. In normal conception, the egg is fertilized by the sperm inside the fallopian tube. The resulting embryo travels through the tube and reaches the uterus 3 to 4 days later. However, if the fallopian tube is blocked or damaged and unable to transport the embryo to the uterus, the embryo may implant in the lining of the tube, resulting in an ectopic pregnancy. The fallopian tube cannot support the growing embryo. After several weeks the tube can rupture and bleed, resulting in a potentially serious situation.
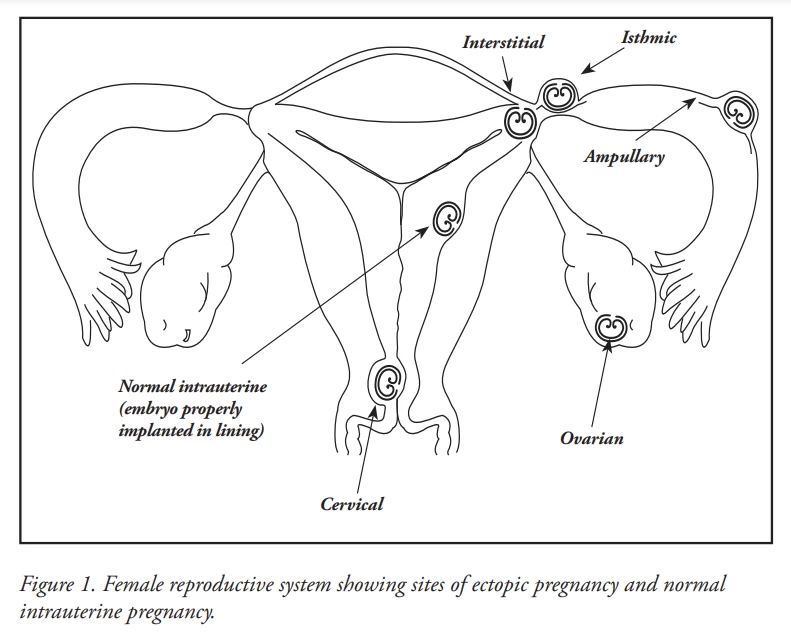
Ninety-five percent of ectopic pregnancies implant in the fallopian tube, but they also can occur in the cervix, ovary (Fig. 1), or even within the abdomen (abdominal pregnancy). Abdominal pregnancies are extremely rare and can progress quite late into the pregnancy before they are discovered. Fetuses that grow in the abdomen who could survive after birth have been delivered, on rare occasions, by laparotomy (abdominal surgery).
Women who have ectopic pregnancies, particularly if they have been attempting to conceive for a long period of time, often ask whether the pregnancy can be removed from the tube and then transplanted into the uterus where it might grow normally. Unfortunately, this is not possible with present medical science.
Causes
Women who already have damaged tubes are more likely to develop an ectopic pregnancy. In fact, 50% of ectopic pregnancies are associated with some degree of tubal disease. Fallopian tube damage commonly results from prior pelvic infection, such as gonorrhea, chlamydia, or other sexually transmitted infections (STIs). Tubal disease also may occur as a result of endometriosis, appendicitis, previous pelvic surgery, or exposure to diethylstilbestrol (DES). The pregnancies of women who conceive with an IUD in place sometimes occur in the fallopian tube. Women who conceive after having a tubal ligation for sterilization, reversal of a tubal ligation, or any other type of tubal surgery also have a higher risk of having an ectopic pregnancy. Women who conceive as a result of fertility drugs or in vitro fertilization (IVF) have a slightly higher risk of having an ectopic pregnancy. For more information on tubal damage and surgery, refer to the ASRM patient information booklet titled, What do i need to know about conceiving after surgery on my fallopian tubes?.
Sometimes, there is no apparent explanation for why an ectopic pregnancy has occurred. However, it is known that once a woman has had an ectopic pregnancy, she has a higher chance of having another one and should be monitored carefully if another pregnancy is attempted or suspected.
Symptoms
Delayed or abnormal bleeding can be an early sign of an ectopic pregnancy. If pregnancy is confirmed, early abnormal levels of human chorionic gonadotropin (hCG), pelvic pain, and/or irregular bleeding in the first weeks of pregnancy can indicate an ectopic pregnancy. If a woman knows or suspects that she is pregnant and has had pelvic or lower abdominal pain, she should consult her physician, even if the pain decreases in severity or stops altogether. Additionally, if a woman has any risk factors for an ectopic pregnancy, including a previous ectopic pregnancy, she should check a home pregnancy test if her period is delayed and consult her physician as soon as she is pregnant. Early detection of an ectopic pregnancy may help minimize the complications associated with ectopic pregnancies and offers the opportunity for other treatment options. Sometimes an ectopic pregnancy is suspected when an ultrasound does not show a pregnancy inside the uterus. Until recently, ectopic pregnancies often were not diagnosed until 6 to 8 weeks into the pregnancy, when a woman was experiencing pelvic pain, irregular vaginal bleeding, possible internal bleeding, and a tender feeling in the pelvis. Under these circumstances, this represented a life-threatening emergency, and major surgery (laparotomy) was required to remove the pregnancy and control bleeding. Fortunately, most ectopic pregnancies are now identified much earlier, often before the woman is even aware of an acute problem. This is largely due to the availability of sensitive hormone testing and ultrasound examinations.
DIAGNOSIS
Human Chorionic Gonadotropin (hCG)
In a normal pregnancy, the blood level of hCG, a hormone produced by the placenta, should double approximately every 48 hours. If this doubling does not occur, this suggests that the pregnancy may not be healthy. It may mean a miscarriage or an ectopic pregnancy. Often measurements of hCG blood levels are repeated to help make the diagnosis.Progesterone
Progesterone levels in the bloodstream rise very early in the course of a pregnancy. Low levels of this hormone are frequently associated with an abnormal pregnancy, such as an ectopic pregnancy or an impending miscarriage. However, progesterone levels alone do not always predict the location or mean the pregnancy is healthy and are not routinely used to diagnose ectopic pregnancy.Ultrasound Examinations
Ultrasound can be used in the first 3 to 5 weeks after conception (as early as 1 to 3 weeks after a missed period) to determine whether or not a pregnancy is inside the uterine cavity. Transvaginal ultrasound is much more sensitive than abdominal ultrasound for this purpose. Ultrasound scans also can show fluid or blood in the abdominal cavity, suggesting bleeding from an ectopic pregnancy. Sometimes, the use of ultrasound, combined with hCG and/or progesterone blood level measurements, can confirm the diagnosis of an ectopic pregnancy without the need for laparoscopy or D&C. Often, it is not possible to see an ectopic pregnancy with ultrasound, and the diagnosis is considered when the pregnancy is not seen in the uterus when specific levels of hCG are also present.Laparoscopy
In some cases, laparoscopy is needed to confirm the diagnosis of an ectopic pregnancy. Sometimes, laparoscopy also can be used to treat ectopic pregnancy. Laparoscopy is an outpatient surgical procedure requiring general anesthesia. A small telescope called a laparoscope is placed into the abdominal cavity through a small incision (cut) in the navel. If necessary, the doctor usually can remove the ectopic pregnancy by placing special instruments through the laparoscope or through small incisions above the pubic area. An overnight hospital stay usually is not necessary following a laparoscopy. For more information on laparoscopy, refer to the ASRM patient information booklet titled, Laparoscopy and Hysteroscopy.Dilation and Curettage (D&C)
If a woman’s blood hormone levels and ultrasounds show that the pregnancy will end in miscarriage or an embryo that has not successfully attached to the uterine wall, the physician may choose to gently scrape out the lining of the uterus. This operation, known as a D&C, can be performed under anesthesia either in the hospital or as an outpatient procedure. A woman’s hCG levels will drop sharply following the removal of a miscarriage. The tissues taken from the uterus also are examined carefully by a pathologist. If pregnancy tissue is seen, an ectopic pregnancy is very unlikely. However, very rarely a double pregnancy can occur, one in the uterus and the other in the fallopian tube (called a heterotopic pregnancy). If there is no evidence of pregnancy tissue or the hCG levels do not drop sharply following a D&C, the presence of ectopic pregnancy must be considered.TREATMENT
Observation Alone
Some ectopic pregnancies resolve without treatment and can be managed by observation alone. This is referred to as “expectant management” and usually is limited to women with early ectopic pregnancies with no symptoms and low serum hCG levels (usually <1,000 IU/L) that decrease without treatment. Treatment of ectopic pregnancy by observation alone can be used only for women who can dependably return for weekly blood hCG levels or sooner if symptoms develop. Women being treated with observation alone should avoid intercourse and strenuous exercise.When hCG levels are <1,000 IU/L and dropping, and pelvic ultrasound is unable to determine the location of the pregnancy, these pregnancies are sometimes referred to as “biochemical pregnancies.” Approximately half are actually ectopic pregnancies, and the rest are intrauterine pregnancies that are destined to end as miscarriages. Observation alone will allow the great majority of these to resolve without incident within a month. If the woman experiences pain or related symptoms, or the hCG levels do not drop appropriately or rise, treatment with the medicine methotrexate or surgery will be necessary.
Medical Treatment
With an early diagnosis of an ectopic pregnancy, medical (non-surgical) treatment often is possible with the drug methotrexate. To be a candidate for methotrexate treatment, a woman needs to be in stable condition with no evidence of internal bleeding or severe pain. She also needs to maintain communication with her physician during the treatment protocol and be able to return for follow-up blood tests after treatment.Methotrexate is a drug that was initially used to treat certain types of cancers, some of which are derived from placental tissue. It is very effective in destroying ectopic pregnancy tissue and allowing it to be reabsorbed by the body. It can also destroy normal pregnancy tissue. Therefore, it is not an option for women with a heterotopic pregnancy. Methotrexate is given as a single intramuscular shot or as a series of shots over several days. Most early ectopic pregnancies can be successfully treated with methotrexate. This often leaves the tube open. Success is based largely on the size of the ectopic pregnancy seen on the ultrasound exam and the level of hCG found on the blood test. Women with large ectopic pregnancies or rapidly rising and/or high levels of hCG (>10,000 IU/L) are less likely to respond to single-dose methotrexate therapy. These women may be considered candidates for multiple-dose methotrexate regimens or surgical treatment. If methotrexate is successful, hCG levels should decrease to zero over the next 2 to 6 weeks. If the hCG levels do not fall, methotrexate treatment may be repeated or the pregnancy may be removed surgically.
There are no known long-term side effects from the use of methotrexate. The short-term side effects are few. The drug can cause temporary ulcers in the mouth and other gastrointestinal areas and can cause temporary changes in liver function. Rare complications include pneumonia. Decreased platelet production, another rare complication, can cause bleeding within 2 weeks after the injection. Any woman with changes in liver blood tests, anemia (low blood counts), or platelet disorders cannot take methotrexate. A woman may have some abdominal pain for a few days due to the resorption of the ectopic pregnancy. Any severe pain needs to be reported to her physician. Women should limit sun exposure during treatment, as methotrexate can cause sensitivity to sunlight and sunburn may occur. When being treated with methotrexate, women should not drink alcohol or take vitamins containing folic acid (folate).
Surgical Treatment
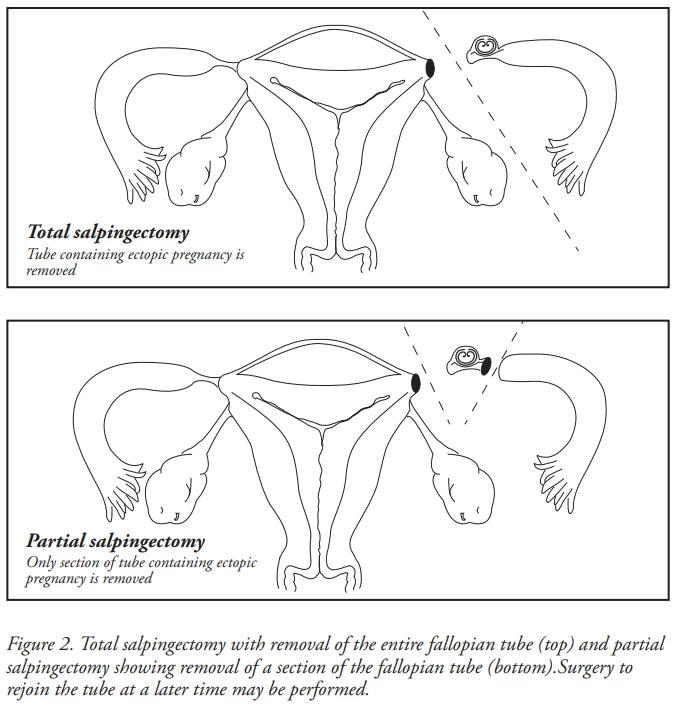
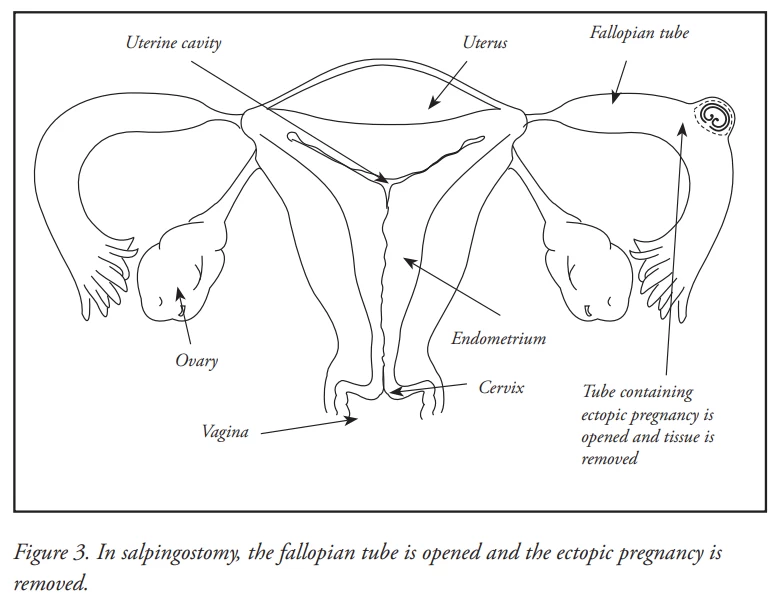
Until the last 20 years, ectopic pregnancies usually were treated by total salpingectomy (removal of the entire tube [Fig. 2]) via laparotomy (major abdominal surgery). Today, most surgeries for ectopic pregnancies are performed by laparoscopy. Laparotomy usually is reserved for those ectopic pregnancies that have ruptured, causing severe internal bleeding, or when there is extensive scar tissue inside the abdomen and pelvis.If the ectopic pregnancy is diagnosed early, before the tube ruptures, a laparoscopic salpingostomy may be performed. In this procedure, the fallopian tube is opened and the pregnancy tissue is removed while leaving the tube in place (Fig. 3). The tube then heals on its own. In about 5% to 15% of cases, some of the ectopic tissue may remain and continue to grow. This may be treated by additional surgery to remove the tube or by using methotrexate therapy. A partial salpingectomy (sometimes called a segmental resection, to remove a middle segment of the tube [Fig. 2]) may be performed when the ends of the tubes (the fimbriae) appear healthy and the ectopic pregnancy is small. If only a small portion of the tube is removed, the tube may be rejoined later using microsurgery. If the fallopian tube is extremely damaged, the ectopic pregnancy is large, or the woman is bleeding excessively, a total salpingectomy is performed. In rare cases when the ectopic pregnancy involves the ovary, a portion of the ovary or the entire ovary may be removed.
Operative Laparoscopy Versus Laparotomy for Ectopic Pregnancy
Up until the late 20th century, all gynecologic, reproductive, and tubal operations were performed by opening the abdomen (called “laparotomy”) using either a “bikini” or “up and down” skin incision several inches long. Women usually remained in the hospital for 2 to 5 days following surgery and returned to work in 2 to 6 weeks, depending on the level of physical activity required. Today, many of these operations can be performed by “laparoscopy,” using a small telescope with a camera and 2 to 4 smaller skin incisions approximately one-quarter to one-half inch long. Following laparoscopy, women generally are able to go home the day of surgery and recover more quickly, returning to full activities in 3 to 7 days.Despite the advantages of laparoscopy, not all surgeries for ectopic pregnancy can be done with this technique. Emergency situations with extensive internal bleeding or large amounts of intra-abdominal adhesions may require immediate laparotomy. Some types of operations also may be too risky to perform laparoscopically, while in others it is not clear that laparoscopy yields results as good as those by laparotomy. Finally, the surgeon’s training, skill, and experience also play a significant role in deciding whether laparoscopy or laparotomy should be used. When considering a pelvic operation, the patient and doctor should discuss the pros and cons of performing a laparotomy versus a laparoscopy, including the surgical risks.
OUTCOME
Emotional Aspects
Ectopic pregnancy is a physically and emotionally traumatic experience. In addition to experiencing the loss of a pregnancy, women may fear the loss of future fertility. Feelings of grief and loss are normal. Sadness, anger, self-blame, guilt, and depression are part of the grieving process and need to be acknowledged and expressed. It can be helpful to share these feelings in a support group, such as RESOLVE or SHARE, or through counseling. Time is necessary for both physical and emotional healing before attempting another pregnancy. For more information on these support groups, consult the Resources section below.SUMMARY
GLOSSARY
Appendicitis. A condition where the appendix (a tubular structure attached to the large colon) becomes infected and inflamed and can be associated with the formation of adhesions in the proximity of the fallopian tube.
Cervix. The lower narrow end of the uterus that connects the uterus to the vagina.
Diethylstilbestrol (DES). A synthetic hormone formerly given during pregnancy to prevent miscarriage. Women born from treated pregnancies can have abnormalities of the reproductive system, including an increased risk of ectopic pregnancy.
Dilation and curettage (D&C). An outpatient surgical procedure during which the cervix is dilated, and the lining of the uterus is scraped out. The tissue is often microscopically examined for the presence of abnormality or pregnancy tissue.
Ectopic pregnancy. A pregnancy that implants outside of the uterus, usually in the fallopian tube. The tube may rupture or bleed as the pregnancy grows and present a serious medical situation.
Embryo. The earliest stage of human development arising after the union of the sperm and egg (fertilization).
Endometriosis. A condition where patches of endometrial-like tissue develop outside the uterine cavity in abnormal locations such as the ovaries, fallopian tubes, and abdominal cavity. Endometriosis can grow with hormonal stimulation, causing pain, inflammation, and scar tissue. It also may be associated with pelvic pain and infertility.
Fallopian tube. A pair of hollow tubes attached one on each side of the uterus through which the egg travels from the ovary to the uterus. Fertilization usually occurs in the fallopian tube. The fallopian tube is the most common site of ectopic pregnancy.
Fertility drugs. Drugs that stimulate the ovaries to produce and mature eggs so that they can be released at ovulation.
Fimbriae. The flared (finger-like) end of the fallopian tube that sweeps over the surface of the ovary and helps to direct the egg into the tube.
Human chorionic gonadotropin (hCG). This hormone is produced by the placenta. Its detection is the basis of most pregnancy tests.
Implantation. The process whereby an embryo embeds in the uterine lining in order to obtain nutrition and oxygen. Sometimes, an embryo will implant in areas other than the uterus, such as in a fallopian tube. This is known as an ectopic pregnancy.
In vitro fertilization (IVF). A method of assisted reproduction that involves combining an egg with sperm in a laboratory dish. If the egg fertilizes and begins cell division, the resulting embryo is transferred into the woman’s uterus where it will hopefully implant in the uterine lining and further develop. IVF may be performed in conjunction with medications that stimulate the ovaries to produce multiple eggs in order to increase the chances of successful fertilization and implantation. IVF bypasses the fallopian tubes and is often the treatment of choice for women who have badly damaged or absent tubes.
Laparoscope. A thin, lighted, telescope-like viewing instrument that is usually inserted through the navel into the abdomen to examine the contents of the pelvic and abdominal cavities. Other small incisions may also be made, and additional instruments inserted to facilitate diagnosis and allow surgical correction of pelvic abnormalities. The laparoscope can be used as both a diagnostic and operative instrument.
Laparoscopy. The insertion of a long, thin, lighted, telescope-like instrument called a laparoscope into the abdomen through an incision usually in the navel to visually inspect the organs in the abdominal cavity. Other small incisions may also be made, and additional instruments inserted to facilitate diagnosis and allow surgical correction of abnormalities. The surgeon can sometimes remove scar tissue and open closed fallopian tubes during this procedure.
Methotrexate. A medication that destroys pregnancy-related tissue and hastens re-absorption of this tissue in a woman with an ectopic pregnancy.
Microsurgery. A type of surgery that uses magnification, meticulous technique, and fine suture material in order to get precise surgical results. Microsurgery is important for certain types of tubal surgery in the female, as well as for vasectomy reversal in the male.
Miscarriage. The naturally occurring expulsion of a nonviable fetus and placenta from the uterus; also known as spontaneous abortion or pregnancy loss.
Ovaries. The two female sex glands in the pelvis, located one on each side of the uterus. The ovaries produce eggs and hormones including estrogen, progesterone, and androgen.
Partial salpingectomy. An operation in which the section of a fallopian tube containing an ectopic pregnancy is removed. This procedure attempts to preserve most of the tube for subsequent re-attachment using microsurgery in order to achieve future fertility.
Pneumonia. Lung inflammation.
Progesterone. A female hormone secreted by the corpus luteum after ovulation during the second half of the menstrual cycle (luteal phase). It prepares the lining of the uterus (endometrium) for implantation of a fertilized egg and also allows for complete shedding of the endometrium at the time of menstruation. In the event of pregnancy, the progesterone level remains stable beginning a week or so after conception.
Salpingectomy. An operation in which one or both of the fallopian tubes are removed.
Salpingo-oophorectomy. Removal of a fallopian tube and ovary together.
Salpingostomy. A surgical procedure in which the wall of the fallopian tube is opened and the ectopic pregnancy is removed. The tubal incision heals spontaneously.
Sexually transmitted infection (STI). An infection, such as chlamydia or gonorrhea, that is transmitted by sexual activity. In the female, some STIs can cause pelvic infections and lead to infertility by damaging the fallopian tubes and increasing the risk of ectopic pregnancy. In the male, STIs can cause blockage of the ductal system that transports sperm.
Transvaginal ultrasound. An imaging technique in which a smooth cylindrical probe that uses sound waves to view organs on a video screen is placed in the vagina.
Tubal ligation. A surgical procedure in which the fallopian tubes are clamped, clipped, or cut to prevent pregnancy.
Ulcer. A lesion (sore) on the surface of the skin or on a mucous surface, usually inflamed. As an occasional side effect of methotrexate therapy, temporary ulcers may form in the mouth.
Ultrasound. A picture of internal organs produced by high-frequency sound waves viewed as an image on a video screen; used to monitor the growth of ovarian follicles, retrieve eggs, or monitor the growth and development of a fetus. Ultrasound can be performed either abdominally or vaginally.
Uterus (womb). The hollow, muscular female organ in the pelvis in which an embryo implants and grows during pregnancy. The lining of the uterus called the endometrium, produces the monthly menstrual blood flow when there is no pregnancy.
Fact Sheets/Booklets
View more fact sheets and booklets written by the ASRM Patient Education Committee.
Menopausal Transition (Perimenopause): What Is It?
The menopausal transition (perimenopause) is the period that links a woman’s reproductive (childbearing) years and menopause.
Osteoporosis
Osteoporosis and osteopenia are conditions of having low bone mass (density).
Optimizing Natural Fertility
Before attempting pregnancy, a woman should make sure she is healthy enough for pregnancy by adopting a healthier lifestyle and taking prenatal vitamins. If she has a medical or genetic condition or risk of one, she should seek advice from a medical professional before conceiving (becoming pregnant)Resources For You
Advocacy Resources
ASRM has prepared resources to help you explain and advocate for reproductive rights and the continuation of in vitro fertilization and other fertility treatments.

Frequently Asked Questions
ASRM's Frequently Asked Questions (FAQ) provides answers to common questions about reproductive health.

Patient Journeys
ASRM has resources and publications to help you through each stage of your journey.

State and Territory Infertility Insurance Laws
One way that ASRM works to improve access to fertility care is by advocating for insurance coverage for reproductive medicine care. All patients should have access to the care they need.
Fact Sheets and Infographics
ASRM produces a series of fact sheets and booklets on various topics related to infertility, reproductive health, and family planning. The fact sheets and booklets are available in English, Spanish, and Chinese.

Reproductive Rights and You
The Dobbs decision has sparked a litany of changes in state laws across the nation, and more are expected. We need your help!

Reproductive Topics
Find all the resources on a specific topic compiled onto a single page.

SART Fertility Experts Podcast
An educational project of ASRM's affiliated society, the Society for Assisted Reproductive Technology (SART), this series is designed to provide up to date information about a variety of topics related to fertility testing and treatment such as IVF.

Patient Education Videos
ASRM and its affiliated society SART have made several videos to explain the sometimes difficult topics related to reproductive medicine.

Terms and Definitions
Find explanations for the meaning behind the doctor-speak you hear when trying to research reproductive medicine topics. ASRM has defined the most popular terms in easy to understand language.

Patient Stories
Read real-life stories from patients who have faced reproductive medicine challenges and come out stronger on the other side.

Fertility in the News
ASRM Press Releases and Bulletins are published by ASRM's Office of Public Affairs to inform the world about important happenings in reproductive medicine and at ASRM.
Ectopic Pregnancy
Side effects of injectable fertility drugs (gonadotropins)
Gonadotropins are fertility medications given by injection that contain follicle-stimulating hormone (FSH) alone or combined with luteinizing hormone (LH). View the fact sheetWhat do I need to know about conceiving after surgery on my Fallopian tubes?
Fallopian tubes connect the ovary (where the eggs are stored and grow) to the uterus (womb), where the fertilized egg develops into a baby (fetus). View the fact sheetHydrosalpinx
The fallopian tubes are attached to the uterus (womb) on the left and right sides. View the Fact SheetDIŞ GEBELİK
Dış gebelik, rahmin dışında gelişen gebeliktir. View the fact sheetEctopic Pregnancy
An ectopic pregnancy is any pregnancy that grows outside of the uterus (womb). In a normal pregnancy, the egg meets the sperm (is fertilized) in the fallopian tube and the embryo (fertilized egg) travels through the tube to the uterus. View the Fact SheetEctopic Pregnancy Infographics
ASRM has prepared infographics to illustrate the subject of Ectopic Pregnancy better. View the InfographicsFind a Health Professional
